
Prostate matters is a not for profit organisation committed to providing free information about prostate issues from leading Clinical Authorities.
Treatment of BPH – Aquablation therapy

Consultant Urological Surgeon
Norfolk and Norwich University Hospital NHS Foundation Trust
Aquablation treatment for enlarged Prostate
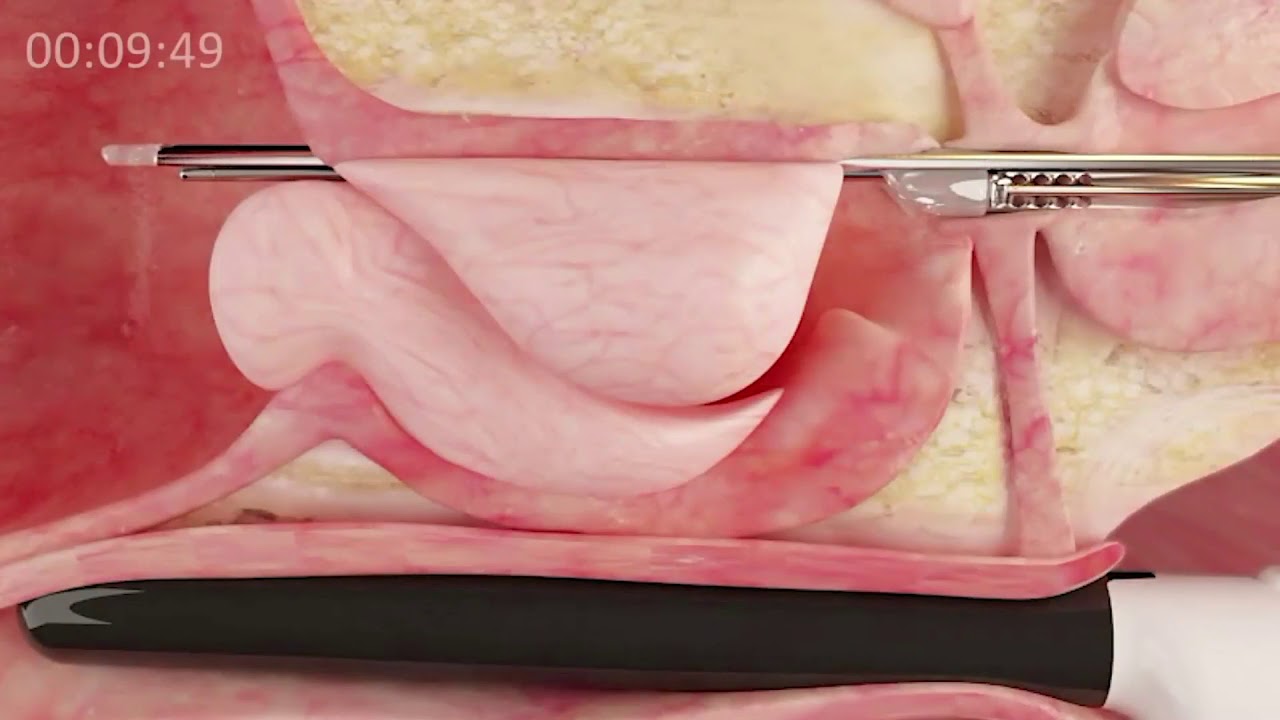
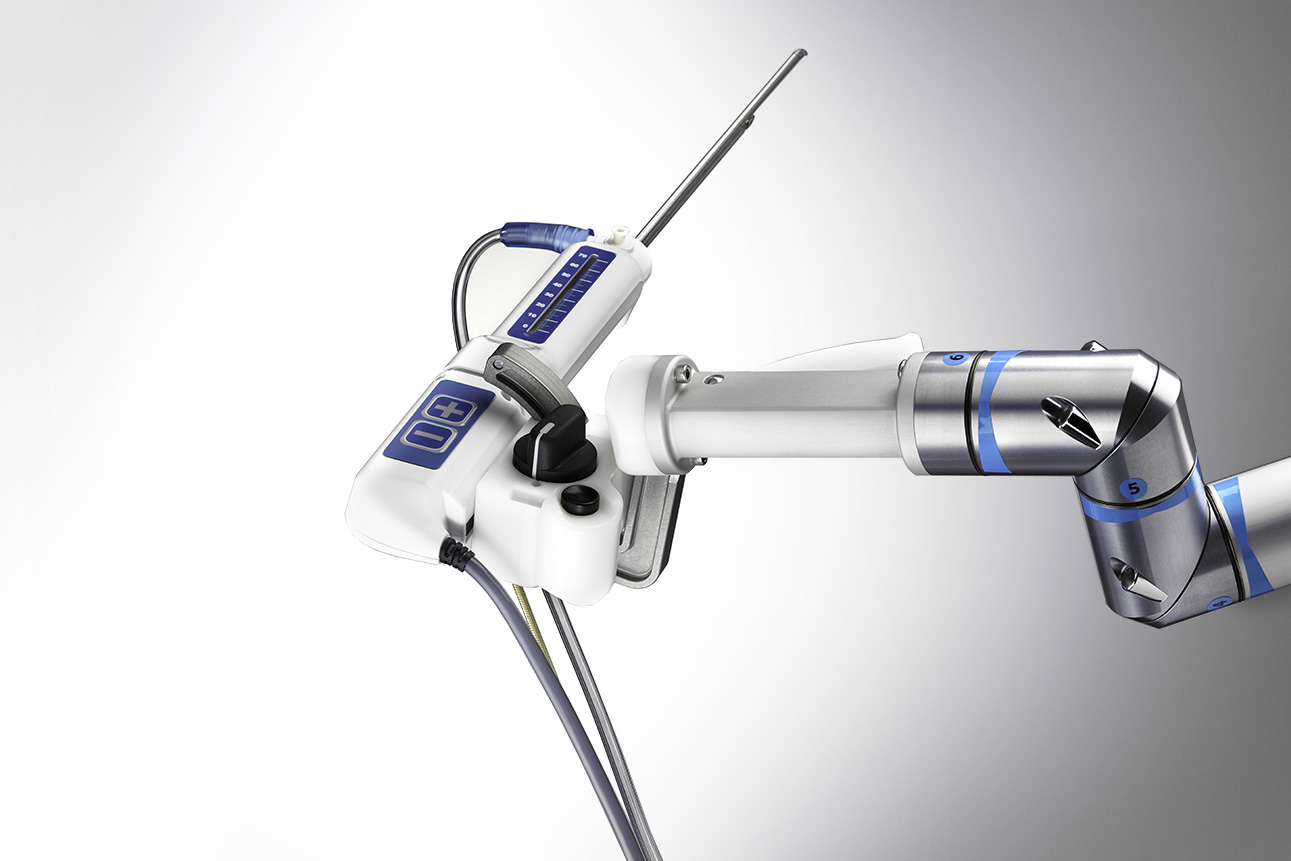
Aquablation treatment for enlarged Prostate or Aquablation therapy of the prostate using the ‘AquaBeam’ Robotic system, is a another novel alternative to TURP for BPH. It was developed by PROCEPT BioRobotics and uses real-time ultrasound scan images in combination with direct visualization to plan and deliver the treatment required. The system uses a high-velocity sterile heat-free waterjet and autonomous robotics, pre-programmed by the Urologist, to remove prostate tissue and create a TURP – like defect through the prostate. I mention TURP as clinical trials have used that procedure as a comparator.
The pre-programming defines the angle of the probe and the depth and duration for firing the water jet. As mentioned, a clinical trial comparing this to TURP in 30-80ml prostates showed that it can achieve symptom and flow improvement to at least as good a level as TURP (the reference standard), with similar re-treatment rate at 5 years. Surgical retreatment was 5% for aquablation at 5 years and 1.5% for TURP, although medical treatment more common in the TURP arm, accounting for the similar reported retreatment rates. (Gilling CJU 2022 ). A further single-arm study of larger prostates up to around 150ml (average size 107ml) showed similar effects, with a 3% surgical retreatment at 5 years and further 6% on medication (Bhojani J Urol 2023). An ongoing study is comparing its effect to that of HOLEP, but is not yet reported.
The procedure is usually performed with the patient under general or spinal anaesthesia. Whilst the ablation time is usually less than 10 minutes, the set up and real time ultrasound guided planning mean that the whole procedure takes about 45 minutes. At the end of the procedure, focal “bladder neck cautery” with a diathermy loop similar to that used for TURP is now recommended to stop bleeding. Once the procedure is complete a 3-way Foley catheter is placed through the penis into the urethra to ‘irrigate’ the bladder. The catheter is usually removed the next day and the patient is typically discharged from hospital once urine has been passed in an adequate fashion, although for some patients, the procedure is now done as a daycase, with the catheter removed at home or in a clinic after 24-48 hours.
The advantages of Aquablation therapy
- A high percentage of men retain normal ejaculatory function (c85%)
- The consistency of treatment delivery
- the speed of the procedure almost whatever the size of the prostate
- It is largely heat free, other than the focal cautery phase, perhaps reducing the risk of complications from thermal injury and damage.
The procedure is very unlikely to result is erectile problems (<1%) and, as noted above, has a low incidence of dry ejaculation at 8%-15% depending on the study
The disadvantages of Aquablation
- There is a higher risk of bleeding than with other techniques, although the introduction of cautery to the procedure has reduced the transfusion rate from 3.9% to 0.8% (Elterman CJU 2021)
- In a similar manner to TURP, it does not remove the entire obstructing “transition zone” of the prostate. While some preservation of tissue may account for the lower rate of dry ejaculation, the trade off in the longer term may be a higher re-treatment when compared, for example with enucleation techniques such as HoLEP. Ongoing studies should address this.
- The procedure always requires catheterization with bladder irrigation and often an overnight stay in hospital, although some surgeons are now delivering this as a daycase procedure
HoLEP Vs Aquablation
The recently published WATER 3 study compared Holmium laser enucleation (HoLEP), which is the standard option for men with larger prostates, compared with Aquablation.
The Aquablation group were split between men with a prostate volume of 150ml or less and men with a prostate volume greater than 150ml.
For men with prostate volumes of 150ml or less, the outcomes were at least as good as for HoLEP, with the added advantage that 85% of men retained a normal ejaculation. This is certainly not the case with HoLEP
However, Aquablation for prostate volumes≥150 ml had high surgical retreatment rates of 24.2% and post operative finasteride drug use of 31.3% .
Therefore Aquablation, among most Urological Surgeons in the UK, is not used for very large prostates greater than 150ml but is becoming the best in class treatment for men with prostates of 150ml or less.


Prostate matters is a not for profit organisation that is committed to providing free expert advice about prostate issues from leading Clinical Authorities
In memory of Riki
PROSTATE MATTERS
FOLLOW US
Copyright Disclaimer: We try to acknowledge copyright as appropriate. If we have used something without acknowledging copyright, this is inadvertent. Please let us know by emailing info@prostatematters.co.uk
Site design and technical development by Webtoys | Intelligent Digital Media