Prostate matters is a not for profit organisation committed to providing free information about prostate issues from leading Clinical Authorities.

Treatment for BPH – Prostate Artery Embolisation (PAE)

Overview by Dr Nigel Hacking
Consultant IR Surgeon and Clinical Lead for UK-ROPE study
Spire Southampton Hospital,
Wellington and Princess Grace Hospitals, London

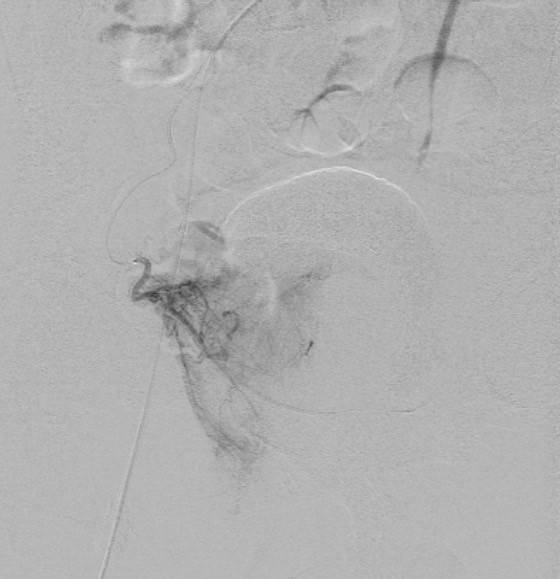
Figure 1:
a.) DSA image of Rt prostate artery b.) DSA of Left Prostate Artery
Prostate embolisation for enlarged prostate, or Prostatic Artery Embolisation (PAE) is a non-surgical way of treating an enlarged prostate by blocking off the arteries that feed the gland and making it shrink. It is performed by an interventional radiologist, rather than a surgeon.
A recent study of 1000 patients in a single cohort center showed that PAE is an effective and safe procedure to treat symptomatic BPH with good results in the short, medium and long term.
Further, recovery time is rapid and the incidence of impotence is very low.
Description of the procedure.
A fine, flexible plastic tube about as thick as a spaghetti strand, a catheter, is inserted into an artery in the right groin, or occasionally the wrist. Using x-ray monitoring to check its position, the catheter is guided into the pelvic arteries and then an even smaller microcather, half the diameter, is manipulated into both your prostate arteries (right and left). An X-ray dye, called contrast medium, is injected down the micro-catheter into these prostate arteries. 3-D CT (Dyna-CT) is used to confirm the safe position of the micro-catheter immediately prior to embolisation. Once the prostate blood supply has been identified and when the micro-catheter is precisely positioned, a fluid containing tiny particles is injected through the catheter. This flows into the prostate arteries and blocks them off.
The particles are made from a plastic-like material called polyvinyl alcohol and are about the size of fine grains of sand. They will remain in your body permanently. In over 30 years of use, they have not shown any harmful effects.
Both the right and the left prostatic arteries are blocked .
Before, during and after the procedure
You do not need to have a general anaesthetic, but you may be given a sedative, which will relax you and make you feel sleepy. You will be given a local anaesthetic in your right groin; the area may also be shaved and sterilised. The procedure can take up to two hours.. Once completed, and the catheter removed, a closure device is inserted to prevent bleeding from the groin. No stitches are required. Patients can mobilize after 1-2 hours and can leave hospital after 4 hours.
A very rare complication is that the particles lodge in the wrong place, so called non-target embolisation. A few self-limiting rectal, bladder and penile ulcers (Less than 1% incidence) have been seen in the first 3000 cases world wide, but not here Dyna-CT has been used.
There is also a 5% chance that the Prostate embolisation for enlarged prostate fails because the arteries are tiny or diseased and so not completely embolised.
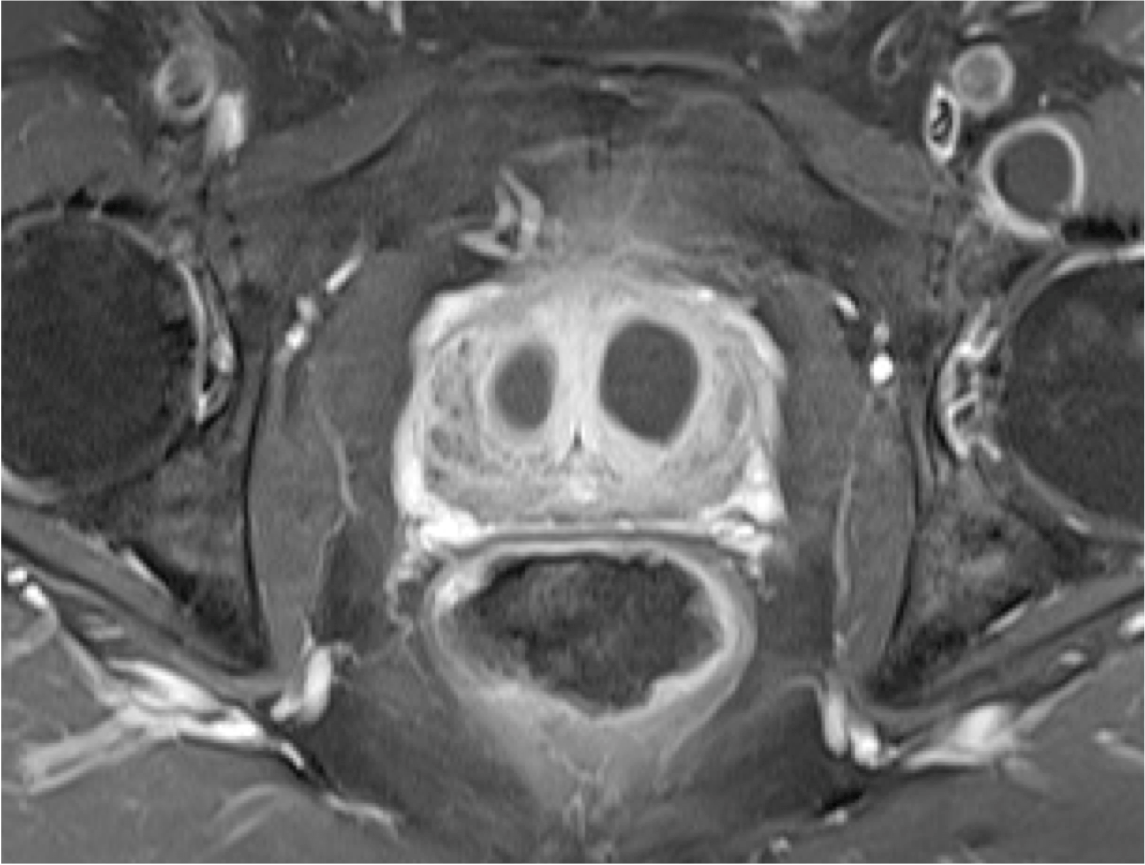
Figure 2. Post contrast MRI showing infarction (death) of the BPH tissue in both left and right lobes of the prostate

Prostate matters is a not for profit organisation that is committed to providing free expert advice about prostate issues from leading Clinical Authorities
In memory of Riki
PROSTATE MATTERS
FOLLOW US
Copyright Disclaimer: We try to acknowledge copyright as appropriate. If we have used something without acknowledging copyright, this is inadvertent. Please let us know by emailing info@prostatematters.co.uk
Site design and technical development by Webtoys | Intelligent Digital Media